


Introduction
Definition of physical activity and sedentary behaviour
All of our daily waking behaviour characterized or fall into one of the following three categories: sedentary behaviour, physical activity and sleep. In 2017 the Sedentary Behaviour Research Network published a paper, which defines each of these behaviours (Tremblay et al., 2017). Figure 1, below, is a summary of these definitions.
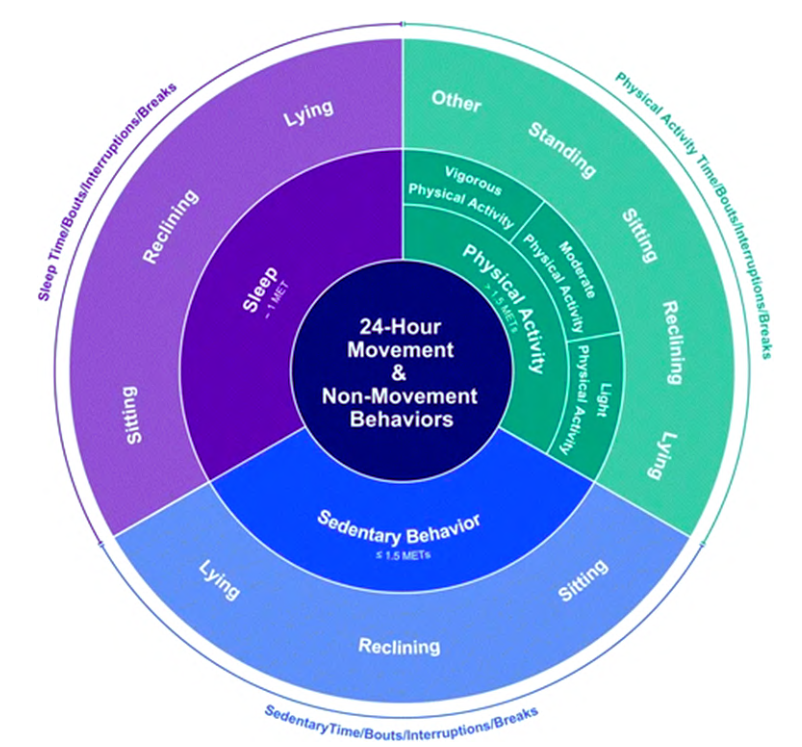
Figure 1. A representation of the three behaviours, which make up a 24-hour day. Each behaviour characterized by an energy expenditure (inner ring) and posture (outer ring). The area each behaviour is allocated is not representative of how much time should be spent in them (Tremblay et al., 2017).
Each behaviour is defined in terms of both posture and energy expenditure. The energy expenditure is expressed in metabolic equivalents of task (METs). METs are used to compare the intensity of different activities to rest (Jetté et al., 1990). 1 MET is equal to 3.5 ml O2/kg/min, which is assumed to be the metabolic rate at rest. All other activities are expressed as a ratio thereof. For example, if an activity has an energy expenditure of 3 METs it uses 10.5 ml O2/kg/min, which is three times more than at rest.
According to physical activity guidelines, an activity is defined as sedentary behaviour if it occurs in a lying, reclining or sitting posture and has an energy expenditure of up to 1.5 METs. Examples of this are sitting at a desk to do homework or lying in bed to watch youtube videos. Physical activity can also occur in a lying, reclining or sitting posture, but is more likely to happen while standing. It can be further divided into light, moderate-to-vigorous physical activity. Based on guidelines on physical activity, activities requiring 1.5 to 3 METs are considered to be light, between 3 and 6 METs they are classified as moderate and above 6 METs they are defined as vigorous. Notably, standing still is classified as light physical activity and not sedentary behaviour. This is an important distinction in sedentary behaviour research. Even though there is no movement, just like in sitting still, keeping the body upright requires more muscle activity and hence increases a person’s energy expenditure (Saeidifard et al., 2018). Likewise, not all sitting behaviour is sedentary behaviour. For example, a study by Howe et al. (2015) showed that playing a video game while seated has a mean MET value of 1.8. Finally, sleep makes up the third category. It is marked by the lowest energy expenditure and happens while sitting, reclining or most frequently, lying down.
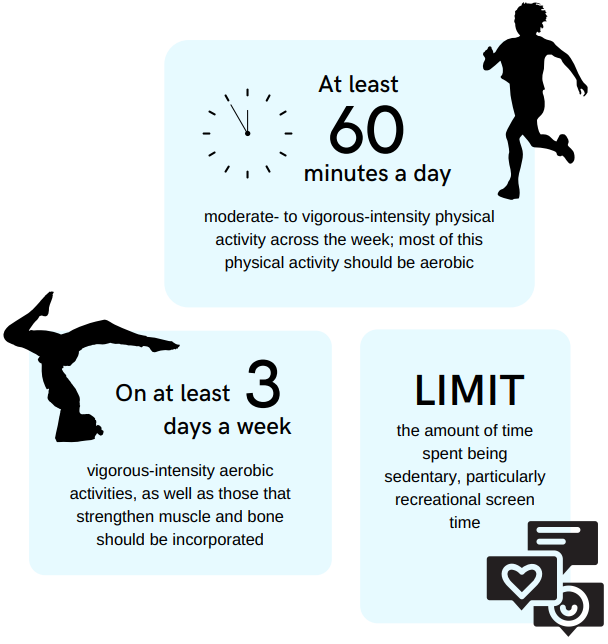
According to the world health organization 2020 guidelines for physical activity of children and adolescents, they should take part in at least 60 minutes of moderate-to-vigorous physical activity a day. Additional benefits are gained from vigorous-intensity activities, as well as muscle- and bone-strengthening exercises on at least 3 days a week. Since 2020 the guidelines also contain recommendations about sedentary behaviour: sedentary activities, especially those that involve screen time, should be kept to a minimum. These recommendations also apply to children and adolescents (i.e., aged 6 to 17 years) with disabilities.
Why is it so important for children and adolescents to be physically active?
The positive effects of physical activity in children and among adolescents on the health outcomes and well-being are manifold (Bull et al., 2020) (Figure 2). Different intensities and types of physical activity affect health in children in different ways. Some of the effects in children and infants are instantaneous and happen after even just a single bout of exercise, whereas others require school children to be active on a more regular basis. Interestingly, research has shown that some of these positive impacts carry over into adulthood. In other words, leading an active life during childhood will benefit the individual for the rest of his or her life (Biddle et al., 2010; Telama et al., 2014).
PA in children and adolescents


Why it is important for a child and adolescent to control physical activity and sedentary behavior: Summary of scientific background
Unfortunately, trends in insufficient physical activity and also overweight and obesity among children and adolescents are increasing and this is important to know how can we have lifestyle-induced health effects in children and adolescents by changing physical activity and body composition using a control on balance of sedentary time and physical activity for children.
A study by NCD Risk Factor Collaboration (2017) analyzed trends in BMI (body mass index) in children and adults from 1975 to 2016 and found that the prevalence of overweight and obesity had increased significantly during this period. In 2016, the global prevalence of obesity among children and adolescents was 5.6% for girls and 7.8% for boys, and the prevalence of overweight and obesity combined was 18.4% for girls and 23.8% for boys.
This increase in overweight and obesity among children and adolescents is concerning because it is associated with numerous lifestyle-induced health effects, such as type 2 diabetes, cardiovascular disease, and certain types of cancer. However, there is evidence to suggest that changing physical activity and body composition through lifestyle interventions can have significant positive health effects in this population.
Martin and colleagues (2017) in a population of children and adolescents found that lifestyle interventions that included both physical activity and dietary changes were effective in reducing BMI and improving cardiovascular risk factors in overweight and obese children and adolescents. The study reviewed 64 randomized controlled trials that included over 5,000 children and adolescents and found that lifestyle interventions resulted in a significant reduction in BMI, as well as improvements in blood pressure, insulin resistance, and lipid profiles.
Rresearch has consistently shown that sedentary behavior is negatively associated with physical activity and fitness in children and adolescents. A study by Biddle and colleagues (2010) found a negative association between physical activity and sedentary behavior, even after adjusting for factors such as age, sex, and socioeconomic status.
Sedentary behavior has also been linked to a range of health indicators in young people. For example, a meta-analysis by Tremblay and colleagues (2011) found that sedentary behavior was associated with increased risk of obesity, high blood pressure, insulin resistance, and lower bone density in children and adolescents.
Moreover, sedentary behavior has been found to be negatively associated with physical fitness in young people. A study by Ortega and colleagues (2008) found that sedentary behavior was inversely related to cardiorespiratory fitness, muscular strength, and flexibility in adolescents.
These findings highlight the importance of reducing sedentary behavior and increasing physical activity levels in young people in order to promote better health outcomes and physical fitness. A review by the World Health Organization (2020) recommends that children and adolescents should engage in at least 60 minutes of moderate-to-vigorous physical activity per day and limit sedentary behavior, including screen time, to less than two hours per day.
Donnelly and colleagues (2009) found that increasing physical activity levels in elementary school children through a school-based physical activity program improved academic performance. The researchers randomly assigned schools to either an intervention group that received additional physical activity programming or a control group that continued with regular programming. The intervention group received an additional 90 minutes per week of physical education and 45 minutes per day of classroom activity breaks. After two years, the intervention group had higher scores on standardized tests of academic achievement, particularly in reading and math, compared to the control group. These findings suggest that school-based physical activity programs may not only promote physical health, but also have positive effects on academic outcomes in children.
But, now let’s discuss a bit about the association between sedentary behavior or insufficient physical activity with health in children and adolescents and benefits of physical activity:
Ekelund and colleagues (2012) found that high levels of sedentary behavior were associated with an increased risk of type 2 diabetes and cardiovascular disease risk factors in children and adolescents. The study followed over 4,000 children and adolescents for up to 6 years and found that those who spent more time being sedentary had higher levels of insulin resistance, higher blood pressure, and higher levels of triglycerides, all of which are risk factors for type 2 diabetes and cardiovascular disease. Sardinha and colleagues (2016) found that regular physical activity was associated with improved bone health in children and adolescents. The study followed over 400 children and adolescents for 3 years and found that those who engaged in regular physical activity had higher bone mineral density and were at a lower risk for fractures compared to their less active peers. Cooper and colleagues (2016) found that physical activity was associated with improved mental health outcomes in adolescents. The study surveyed over 7,000 adolescents and found that those who engaged in regular physical activity had lower levels of depressive symptoms and better overall mental health compared to their less active peers.
In summary considering physical activity and health indicators and recommendations for children, it should be say that physical activity has numerous health benefits for children and adolescents, including improved cardiorespiratory fitness, muscular strength and endurance, bone health, and mental health outcomes. Additionally, based on guidelines for children and youth regular physical activity can help to reduce the risk of chronic diseases such as obesity, type 2 diabetes, and cardiovascular disease.
Finally, let’s take a look at some guidelines regarding 24-hour movement guidelines for children and adolescents.
The Canadian 24-Hour Movement Guidelines for canadian children and youth recommend that children aged 5 to 17 years engage in at least 60 minutes of moderate to vigorous physical activity per day, accumulate at least several hours of light physical activity throughout the day, limit recreational screen time to no more than 2 hours per day, and aim for 9 to 11 hours of uninterrupted sleep per night for 5-13 year olds and 8-10 hours for 14-17 year olds. The guidelines also recommend that children should not be sedentary for extended periods of time and should break up long periods of sitting with activity.
Furthermore, the World Health Organization recommends that children and adolescents engage in at least 60 minutes of moderate-to-vigorous physical activity each day. This can include activities such as running, cycling, swimming, and sports, as well as structured exercise programs and active transportation (e.g., walking or biking to school). In addition to regular physical activity, reducing sedentary behavior (e.g., screen time-based sedentary, playing video games) is also important for promoting better health outcomes in children and adolescents.
The importance of measuring physical activity and sedentary behaviour among children and adolescents
There are various reasons why it’s important to know how much is childrens’ sedentary behavior and physical activity and how they correlates with different health in children and adolescents. It can help form national and international (i.e., global physical activity) recommendations, such as the WHO guidelines mentioned earlier, as well as inform political decision-making. Measuring level of physical activity is also important for assessing whether different population groups are meeting the recommendations. If they are not, it can help develop interventions. After an intervention has been carried out, the same methods can be used to test its short- and long-term success. (Kallio et al., 2022)

Many of us are familiar with activity trackers, as they have become increasingly popular in recent years for assessment of youth physical activity and physical inactivity. Besides activity trackers, there are also other methods which can be used. They typically fall into one of two categories: subjective or objective. Subjective methods, for example, include questionnaires, diaries and interviews. Objective methods, on the other hand, are often device-based and include heart rate monitors, GPS trackers and accelerometers. This article will give a brief introduction to all of these methods, but will especially be focusing on accelerometry. That’s because during the last 20 years accelerometers have been gaining more and more traction
and are currently the most popular assessment tool in physical activity and sedentary time research (Troiano et al., 2014).
Which method for measuring physical activity and sedentary behaviour among children and adolescents should I choose?
The answer to this question largely depends on your research question, as well as your expertise, budget and time-availability. There are many methods to choose from and they all have their own advantages and disadvantages. A summary of this is shown in Table 1a and b.
Table 1a. The most common subjective methods of measuring physical activity and levels of sedentary behaviour (Kallio et al., 2022)
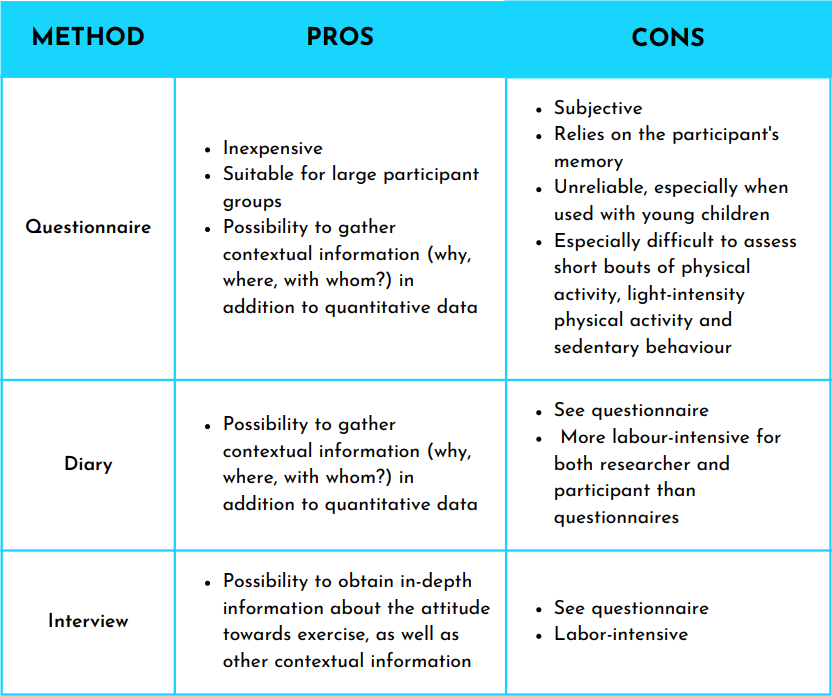
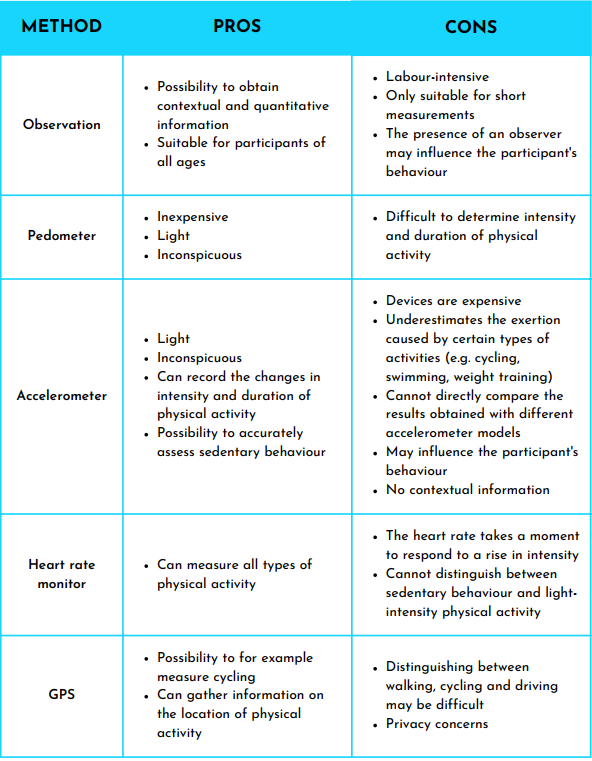
Table 1b. The most common objective methods of measuring physical activity and levels of sedentary behaviour (Kallio et al., 2022)
A couple of key points to remember: guidelines on physical activity and sedentary behaviour for children and adolescents
Before taking a closer look at the individual methods, there are a couple of key points worth mentioning. These are factors that are important to keep in mind, no matter which method you end up choosing for your own survey for children and adolescents.
What are we measuring in those school-aged children and youth?
First, let’s talk about what we are trying to measure in the first place. In measures of children’s physical activity and sedentary behaviour research we are typically interested in how much of a certain activity a person is performing during a given time (e.g. day, week, month, year). This is known as the volume and can be calculated by multiplying how often this activity takes place with intensity and duration. The volume of physical activity can further be divided into three categories: light-, moderate- and vigorous- intensity physical activity. We often want to know how much time a person spends in each of these categories, because each category is associated with slightly different health indicators in school-aged children and adolescents.
Another outcome measure of interest is the patterns of physical activity and sedentary behaviour. For example, we might not only want to know how many minutes per day children are sitting down, but in what pattern they are acquiring this total volume. Are they sitting for many hours on end or are the sitting bouts typically short and interspersed with some movement? Besides quantitative data, we might also want to gather contextual information. We gather contextual data by asking questions, such as “with whom is this behaviour taking place, where and why”? Answers to these questions can help us develop better interventions and recommendations, because all our activities are limited by contextual factors (Troiano et al., 2014).
How are we measuring?
So now that we know what we are interested in measuring, we are ready to tackle the next question: how? Ideally, we would choose a method that is inexpensive, easy to use, accurately captures the information we are interested in and can be applied to as many participants as possible. Unfortunately, it is unlikely that a single method can meet all those needs. Very often a method either leans more towards accuracy or towards user-friendliness (Kallio et al., 2022). User-friendliness in this instance means that it is inexpensive, can be used on many participants and that the data is simple to acquire and analyse. A depiction of where different methods fall on this spectrum can be seen in Figure 3.

Figure 3. Different methods that can be used in physical intensity and sedentary behaviour research to estimate energy expenditure and movement intensity. The choice is a balancing act between accuracy and user-friendliness (Kallio et al.,
2022).
Furthermore, it is important to remember that no matter how accurate a method is, it will never give a 100% true representation of reality. Each method has its own sources of error and is influenced by the decisions of the researcher and how the participants want to present themselves (desirability bias). The results will thus at best be an estimate. Some population groups, such as children with disabilities, are also frequently underrepresented in research. This means that we do not know how valid different methods are when applied to these groups. (Kallio et al., 2022)
Finally, in some instances it might make sense to use a combination of methods so they can balance out each other’s strengths and weaknesses. For example, accelerometers excel at capturing movements and a lack thereof on a second-by-second basis, but they have a hard time distinguishing between sedentary behaviour and sleep. Researchers could thus ask participants to keep a sleep diary (Aunger & Wagnild, 2022; Edwardson et al., 2017). Many of the objective methods also fail to capture contextual information, which researchers might be interested in. One way to alleviate this problem is to supplement the device-based data with questionnaires or interviews.
Validity and comparing results
When reading different studies and designing your own, it’s important to keep in mind that results acquired with different methods should not be directly compared. Indeed, sometimes even the same methods are not comparable. For example, accelerometer data is heavily influenced by wear location, device settings, algorithms used to analyse the data and so on (Migueles et al., 2017). This means that even if the same device was used in two different studies, caution should be used when comparing the results. Another factor, which influences the results is the target population. Some methods may
accurately capture the physical activity of healthy adults but will underrepresent how active a group of adolescents is. Some research has also shown that the point in time has an effect. For example, Finnish children tend to move 8% less during the autumn than they do in the springtime (Kulmala 2012). This makes data collected at different time points less comparable. For these reasons, it is important to read a study’s methodology section carefully and when designing your own, find validation studies that best fit your population group, as well as method of choice.
Subjective methods of measuring physical activity and sedentary behavior in school children and adolescents aged 5–17
Most of the methods falling into this category are so called self-report methods. They include different types of questionnaires and diaries, as well as interviews. These methods are based on the individual’s point of view and their ability to remember.

Questionnaires
Questionnaires are a popular choice for studies that include a lot of participants. They help us answer questions, such as “which population group would benefit most from a physical activity intervention?” and “how many children who go to school in this district are meeting the physical activity recommendations?”. Questionnaires indeed have many advantages. They are inexpensive and because most of the work can nowadays be done digitally, they are easier to distribute and analyse than ever before. They provide useful information on the context of movement, including company, environment and
enjoyability, all of which are factors that influence how often a child likes to move. Unlike device-based methods, questionnaires also allow researchers to take a look at the past, by asking about past behaviours. Even though the accuracy may be limited, it can still provide an important point of reference. A further advantage of questionnaires is that they can capture movement types, that activity trackers may struggle to (Niemi et al., 2020). These include swimming, cycling and weightlifting. (Kallio et al., 2022)
Diaries
Another popular self-report method is the diary. This method is more labour-intensive for both the participant and the researcher. However, it has the advantage of providing more accurate results than questionnaires. Most people
find it easier to remember what they did on the same day than a week or more ago.
Interviews
The third method, which belongs to this category, is the interview. It requires a lot of work from the researcher, which
oftentimes limits the number of participants. The advantage of an interview is that it can be tailored to the interviewee
and that it excels at gathering in-depth contextual information. Interviews thus allow researchers, for example, to explore
intrinsic and extrinsic motivational factors, which influence how active a person is.
Most of children’s moderate and vigorous-intensity physical activity happens in bouts of 10 seconds or less. This type of
movement is impossible to remember.
Limitations
All three methods come with their own set of limitations, some of which particularly pertain to children and adolescents. For example, questionnaires and diaries are not suitable for children under the age of 10, since they cannot reliably estimate their own physical activity levels (Baranowski et al., 1984; Chinapaw et al., 2010). Additionally, the way children move is often intermittent and transitory. While adults typically perform a certain type of activity for several minutes or more, most of children’s moderate and vigorous-intensity physical activity happens in bouts of 10 seconds or less (Baquet et al.,
2007). This type of movement is essentially impossible to remember and thus accurately quantify with self-report methods. Light-intensity physical activity and sedentary behaviour are also difficult to capture with these methods. If that is the aim
then it might be more beneficial to ask about specific types of activities, such as doing homework or spending time on social media, than broadly asking about light-intensity activities and sedentary behaviour (Kallio et al., 2022).
Objective methods: measuring 24-hour movement behavior in children and adolescents aged 5–17 years
Most objective methods, except for direct observation, are device-based. Devices, such as heart rate monitors, GPS trackers, pedometers and accelerometers can be used individually or in combination with each other, in order to track a person’s physical activity. Many of them have become cheaper and more readily available during the last decades and hence have become an increasingly popular choice in physical activity and sedentary behaviour research. However, since they are still more expensive and labour-intensive than questionnaires, the sample sizes that can typically be studied with these devices are limited. It is also important to keep in mind that while these methods do capture the total volume of physical activity and sedentary behaviour more accurately than the objective methods, they are still not a 100% accurate. All devices
have their own sources of error and a researcher’s decisions about what settings to use and how to analyse the data also influence the outcome (Arvidsson et al., 2019). The following sections are an introduction to some of the devices that can be used in field of assessment of physical activity and sedentary time. Accelerometers will be covered a little bit more in depth in the next section.

Heart rate monitors
Heart rate monitors are often seen in combination with other devices, since heart rate is not perfectly correlated with energy expenditure and thus exercise intensity. For example, a person’s heart rate during sedentary activities and light-intensity physical activities are usually quite similar, even if the energy expenditure of the latter is higher. This means that heart rate monitors are a poor choice if one wants to distinguish between those two types of behaviours (Brage et al., 2015). Heart rate monitors also always require a personal calibration to correlate the individual’s heart rate with different movement intensities. The advantage of heart rate monitors is that they can help estimate stress and recovery (Moilanen & Vehviläinen, 2019).

GPS trackers
GPS trackers are especially useful if the goal is to measures of physical activity commutes to and from school. Different algorithms have been developed, which can automatically distinguish between different modes of transportation, such as walking, cycling or taking the bus/being driven. The disadvantages of GPS trackers are that they only work outside and that currently there are no valid methods of correlating energy expenditure with walking or cycling.
Pedometers
Due to their low expense and ease of use, pedometers have been a popular tool in physical activity research. In addition to that, counting steps is a simple way to conceptualize how much a person is moving throughout the day. Because pedometers
have been so widely used, step-based recommendations exist for various age groups (Tudor-Locke et al., 2011). For example, in children 60 minutes of movement is roughly equal to 9000 steps (Adams et al., 2013). The biggest disadvantage of pedometers is that they cannot assess physical activity intensity. At best, they can provide a rough estimate. Coupled with the development of acceleration-based activity trackers during the last two decades, this has meant that pedometers are no longer as popular a tool in physical activity research (Bassett et al., 2017).
Focus: Accelerometers
Next, we will take a closer look at accelerometers. This section will be more extensive than the previous ones, because accelerometers are currently the most popular physical activity and sedentary behaviour research tool. If you would like even more information on these devices, please have a look at our other ebook, entirely dedicated to accelerometers. Since most activity trackers are based on measuring acceleration, the terms accelerometer and activity tracker will be used interchangeably. Most research-grade accelerometers measure and record accelerations taking place along three orthogonal axes. It is assumed that the accelerations are entirely caused by muscle contractions. This assumption allows researchers to correlate acceleration data with energy expenditure and movement intensity, two important outcome measures of
this type of research. The lack of acceleration in turn is an indication that the person is either sedentary or sleeping.
The benefit of accelerometers, compared to self-reported physical activity, is that they can track activity on a second-by-second basis and do not rely on a person’s memory. This is especially helpful when the target population is children. Many models, nowadays, are also waterproof, which means that they can be worn around the clock. This not only means
less work for the participant, but it also opens up the opportunity of tracking sleep (Troiano et al., 2014). While this is still an area under development, some promising results have been achieved with wrist-worn accelerometers.
Typically, the challenge in tracking sleep is assessing where sedentary behaviour ends and sleep starts. To circumnavigate this problem, researchers can ask participants to write down when they went to sleep and woke up, to ask the parents if the target population is very young, or to use other monitors in addition to the accelerometers (Aunger & Wagnild, 2022; Edwardsson et al.,2017).
While accelerometers are seemingly easy to use, it is important not to oversimplify the process. When working with accelerometers many decisions are made along the way, which will influence the results. Before starting the measurements, a suitable device, sampling frequency and wear-location need to be chosen. After the data collection period is over the data needs to be uploaded, which will either be in the form of raw acceleration signals or proprietary activity counts. When analysing the data different filters can be applied, the signals can be summed over different epoch lengths and
various algorithms can be used. These algorithms are either supplied by the device company itself, or they can be open-source. Some of these decisions are predetermined by the device company itself, while others are entirely up to the researcher him- or herself. It is important that the researcher pays careful attention to these decisions both when reading the literature and when designing a study.
While accelerometers are seemingly easy to use, it is important not to oversimplify the process.

The next section will be a short discussion about one of the most important decisions that has to be made along the way: wear location. This will be followed by a note on epoch lengths, since this is a particularly important factor when measuring children.
Wear location
Accelerometers can be worn on different body parts. The most common ones are the wrist, hip/waist and thigh. Each of these locations comes with its own advantages and disadvantages (Arvidsson et al., 2019).

WRIST
Wrist-worn activity trackers often provide high compliance. For example, a study by Scott et al. (2017) revealed that adolescents preferred wearing the accelerometer on the wrist than the hip, because they found it “less uncomfortable” and “less embarrassing”. This in turn led to more valid recordings that could then be analysed. The downside of this wear location is that movements of the wrist are not always related to movements of the lower body or centre of mass. Wrist-worn accelerometers hence struggle to detect postures (e.g. sitting, standing), changes between them and also movements, where the upper body remains relatively still (Montoye et al., 2016; Rosenberger et al., 2013; Suorsa et al., 2020). An example for this is cycling. Also standing may be incorrectly classified as sedentary behaviour. On the flipside, wristworn accelerometers may overestimate the intensity of activities that include a lot of movement of the arms, but little lower body activity.
Adolescents find wrist-worn trackers less uncomfortable and less embarrassing than hip-worn devices.
HIP OR WAIST
The waist has been a very popular attachment site for activity trackers. Since it is close to the body’s centre of mass, it is generally a good representation of the body’s movements (Rosenberger et al., 2013). It is also a fairly comfortable and natural
attachment place. Trackers can be attached with a belt clip or an elastic belt and they tend to stay in place. While the wrist overestimates energy expenditure of activities performed while sitting and moving the arms, the waist location underestimates these. It also struggles to detect postures and changes between them and activities, such as cycling and weight training (Edwardson et al., 2016). A further disadvantage is that many of the waist-worn trackers are not waterproof and hence need to be taken off before going to the shower. Generally, a 24-hour protocol is preferred with activity
trackers, because participants often forget to put the devices back on, which leads to less data. It also increases the participant burden and may increase desirability bias if they constantly need to deal with the tracker rather than being able to just forget about it.
THIGH
Thigh-worn trackers tend to provide the most accurate results. Not only do they detect accelerations caused by locomotion, but they are also able to differentiate between certain types of postures. For example, a thigh-worn device is able to distinguish between sitting and standing, which is important for correctly classifying activities as either sedentary behaviour or light-intensity physical activity. Some trackers are also able to recognise cycling. Additionally, most thigh-worn devices are waterproof and can hence be worn around the clock. The downside of these devices is that they can cause skin irritations in those with sensitive skin. In a study involving adolescent girls around 50% reported discomfort and that they would not want to wear the device again (Shi et al., 2019). One way to get around this problem is to attach the device with an elastic
strap. Some trackers can even be put into the front pocket, albeit they are less accurate this way (Yang et al., 2018). Another issue is that while thigh-worn devices can differentiate between sitting and standing, making a distinction between sitting and lying is more difficult if not impossible. If researchers would like to accurately distinguish between those two, they should consider attaching an accelerometer both to the thigh and lower back.
OTHER LOCATIONS
Some manufacturers have also developed activity trackers that are meant to be worn on other body parts, including the lower back, chest, ankle, upper arm and head. Typically, they serve a specific purpose. For example, ankle-worn sensors are often used to analyse running technique. While they can also be used to measure more general physical activity, there are
more resources for the wear locations mentioned above.
Epoch length
The acceleration signals recorded by a device are often filtered and summed over a specific time period, called epoch. The most common epoch length is 60 s, but also 1 s, 5 s, 15 s and 30 s epochs can be found in the literature (e.g. Hwang et al., 2018). While summing the acceleration in this way decreases the storage space needed and can hence increase the length of the data collection period, it does change the results. Edwardson and Gorely (2010) investigated the effect different epoch lengths have on sedentary behaviour and physical activity classification in children and adolescents. They reported that it had a significant effect on how much time spent in sedentary behaviour, light-intensity, as well as vigorous-intensity physical activity. Children tend to move in more spontaneous and intermittent ways (Berman et al., 1998). Within one minute they might switch from sitting to full out sprinting to walking again. To truly capture these variations, rather than just an average, it is recommended that researchers use shorter epoch lengths when assessing children (Edwardson and Gorely, 2010).
Consumer- vs. research-grade devices
Consumer-grade activity trackers are those that have been developed for the general population. They are often wrist-worn or integrated into the phone and allow an individual to track their everyday activities, sleep quality and/or recovery. Many of
them are based on accelerometry, but also include other sensors, such as GPS. While these devices are hugely popular and boast many advantages, such as attractive prices and designs, it is recommended that researchers do not use these for their studies. One of the prime reasons for this is that the analysis methods are almost always proprietary (Henriksen et al., 2018). This means that the researcher has no idea how the data was analysed. It is also possible for the companies to change those algorithms without letting the consumer know, which makes data collected at different time points impossible to compare. Additionally, the market tends to change faster than validation studies can be conducted. By the time a particular model has been validated, it is very likely that it is no longer on the market. For these reasons researchers are encouraged to choose research-grade devices. These devices typically let the researchers choose their own device settings and analysis methods, the raw data is often accessible and especially the most popular models are well-validated.
A special note about children with disabilities
Children with disabilities are less physically active, and are at a higher risk for metabolic diseases like obesity and diabetes. Activity trackers can be a good method to measure physical activity and sedentary behavior in these children.
It is important that all children and adolescents are included and represented in physical activity and sedentary behaviour research. Indeed, there are nowadays international treaties, as well as national laws in certain countries, which even require
this (Kallio et al., 2022). To do so the methods often need to be adapted. For example, questionnaires have been developed for children with cognitive disabilities. They use simple language and include a lot of pictures. It is also possible to measure the activity of wheelchair users by attaching one accelerometer to the chair and one to the person (Karinharju et al., 2021). By getting creative, we as researchers can contribute greatly to these children feeling included and getting important feedback about the physical activity and sedentary behaviour.
Key messages
- Being physically active during childhood has a positive effect on adulthood
- Measuring children’s and adolescents’ physical activity and sedentary behaviour is needed for ensuring that they are meeting the recommendations, for forming guidelines, political decision making and designing interventions
- Many different methods can be used to track physical activity and sedentary behaviour, each with its own pros and cons
- Which method you choose depends on your research question, budget, timeavailability and expertise
- Make sure that your method of choice has been validated for your population group. Take extra care if the population group is typically underrepresented in research (e.g. children with disabilities)
- Consumer-grade devices are not suitable for scientific research, especially if the study is a longitudinal one
- The time of year may affect how active the children are. Take this into consideration if you are comparing different points in time
- Results obtained with different methods cannot be directly compared
- Children with disabilities have a right to be included in scientific research and to receive feedback about their physical activity and sedentary behaviour
Frequently asked questions about this topic:

A systematic way of assessing physical activity outcomes in children
- With Fibion you are getting a system that makes data collection as easy as it can be!
- The system is designed for children and professionals working with children.
- The feedback is presented by a polar bear, which makes it engaging, as well as educational.
- Scientifically validated data about physical activity, sedentary behaviour, and energy expenditure are automatically created.
- When using the Fibion SENS device you will also have access to raw acceleration data.
For more information go to https://fibionkids.fibion.com/
References
Adams, M. A., Johnson, W. D., & Tudor-Locke, C. (2013). Steps/day translation of the moderate-to-vigorous physical activity guideline for children and adolescents. International Journal of Behavioral Nutrition and Physical Activity, 10, 1–11. https://doi.org/10.1186/1479-5868-10-49
Arvidsson, D., Fridolfsson, J., & Börjesson, M. (2019). Measurement of physical activity in clinical practice using accelerometers. Journal of Internal Medicine, 286(2), 137–153. https://doi.org/10.1111/joim.12908
Aunger, J., & Wagnild, J. (2022). Objective and subjective measurement of sedentary behavior in human adults: A toolkit. American Journal of Human Biology, 34(1). https://doi.org/10.1002/ajhb.23546
Baquet, G., Stratton, G., Van Praagh, E., & Berthoin, S. (2007). Improving physical activity assessment in prepubertal children with high-frequency accelerometry monitoring: a methodological issue. Preventive medicine, 44(2),
143–147. https://doi.org/10.1016/j.ypmed.2006.10.004
Baranowski, T., Dworkin, R. J., Cieslik, C. J., Hooks, P., Clearman, D. R., Ray, L.,Kay Dunn, J., & Nader, P. R. (1984). Reliability and Validity of Self Report of Aerobic Activity: Family Health Project. Research Quarterly for Exercise and Sport, 55(4), 309–317. https://doi.org/10.1080/02701367.1984.10608408
Bassett, D. R., Toth, L. P., LaMunion, S. R., & Crouter, S. E. (2017). Step Counting: A Review of Measurement Considerations and Health-Related Applications.Sports Medicine, 47(7), 1303–1315. https://doi.org/10.1007/s40279-016-0663-1
Berman, N., Bailey, R., Barstow, T. J., & Cooper, D. M. (1998). Spectral and bout detection analysis of physical activity patterns in healthy, prepubertal boys and girls. American Journal of Human Biology, 10(3), 289–297.
https://doi.org/10.1002/(SICI)1520-6300(1998)10:3<289::AID-AJHB4>3.0.CO;2-E
Biddle, S. J. H., Pearson, N., Ross, G. M., & Braithwaite, R. (2010). Tracking of sedentary behaviours of young people: A systematic review. Preventive Medicine, 51(5), 345–351. https://doi.org/10.1016/jypmed.2010.07.018
Brage, S., Westgate, K., Franks, P. W., Stegle, O., Wright, A., Ekelund, U., & Wareham, N. J. (2015). Estimation of free-living energy expenditure by heart rate and movement sensing: A doubly-labelled water study. PLoS ONE, 10(9).
https://doi.org/10.1371/journal.pone.0137206
Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., Carty, C., Chaput, J. P., Chastin, S., Chou, R., Dempsey, P. C., Dipietro, L., Ekelund, U., Firth, J., Friedenreich, C. M., Garcia, L., Gichu, M., Jago, R., Katzmarzyk, P. T., … Willumsen, J. F. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine, 54(24), 1451–1462. https://doi.org/10.1136/bjsports-2020-102955
Chinapaw, M. J. M., Mokkink, L. B., Poppel, M. N. M. Van, Mechelen, W. Van, &Terwee, C. B. (2010). Physical Activity Questionnaires for Youth A Systematic Review of Measurement Properties. Sports Medicine, 40(May 2009), 539–563.
Donnelly, J. E., Hillman, C. H., Castelli, D., Etnier, J. L., Lee, S., Tomporowski, P., … & Szabo-Reed, A. N. (2016). Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Medicine and science in sports and exercise, 48(6), 1197-1222.
Edwardson, C. L., & Gorely, T. (2010). Epoch Length and Its Effect on Physical Activity Intensity. Medicine & Science in Sports & Exercise, 42(5), 928–934. https://doi.org/10.1249/MSS.0b013e3181c301f5
Edwardson, C. L., Rowlands, A. V., Bunnewell, S., Sanders, J., Esliger, D. W.,Gorely, T., O’Connell, S., Davies, M. J., Khunti, K., & Yates, T. (2016). Accuracy of Posture Allocation Algorithms for Thigh- and Waist-Worn Accelerometers. Medicine and science in sports and exercise, 48(6), 1085–1090. https://doi.org/10.1249/MSS.0000000000000865
Edwardson, C. L., Winkler, E. A. H., Bodicoat, D. H., Yates, T., Davies, M. J.,Dunstan, D. W., & Healy, G. N. (2017). Considerations when using the activPAL monitor in field-based research with adult populations. Journal of Sport and Health Science, 6(2), 162–178. https://doi.org/10.1016/j.jshs.2016.02.002
Henriksen, A., Haugen Mikalsen, M., Woldaregay, A. Z., Muzny, M., Hartvigsen,G., Hopstock, L. A., & Grimsgaard, S. (2018). Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer
Wrist-Worn Wearables. Journal of medical Internet research, 20(3), e110.https://doi.org/10.2196/jmir.9157
Howe, C. A., Barr, M. W., Winner, B. C., Kimble, J. R., & White, J. B. (2015). The Physical Activity Energy Cost of the Latest Active Video Games in Young Adults. Journal of Physical Activity and Health, 12(2), 171–177. https://doi.org/10.1123/jpah.2013-0023
Hwang, J., Fernandez, A., & Lu, A. (2018). Application and Validation of Activity Monitors’ Epoch Lengths and Placement Sites for Physical Activity Assessment in Exergaming. Journal of Clinical Medicine, 7(9), 268. https://doi.org/10.3390/jcm7090268
Jetté, M., Sidney, K., & Blümchen, G. (1990). Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clinical Cardiology, 13(8), 555–565. https://doi.org/10.1002/clc.4960130809
Kallio, J., Kulmala, J., & Tammelin, T. (2022). Näkökulmia lasten ja nuorten liikkumisen mittaamiseen ja tulosten tulkintaan.
Karinharju, K., Clanchy, K., Gomersall, S., Trost, S., & Tweedy, S. (2021). Systematic review of device-based motion sensors for monitoring physical activity in community-dwelling manual wheelchair users. In Online ISAPA 2021 Quality partnerships in Adapted Physical Activity: Stronger Together! Book of abstracts (p. 112).
Kulmala, J., Hakonen, H., Siekkinen, K., & Tammelin, T. (2012). Seasonal variation in objectively measured physical activity among Finnish boys and girls aged 7 to 15 years. 7th European Youth Hearty Study Scientific Symposium.
Migueles, J. H., Cadenas-Sanchez, C., Ekelund, U., Delisle Nyström, C., MoraGonzalez, J., Löf, M., Labayen, I., Ruiz, J. R., & Ortega, F. B. (2017). Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Medicine, 47(9), 1821–1845. https://doi.org/10.1007/s40279-
017-0716-0
Moilanen, N., & Vehviläinen, H. (2019). Aktiivisuutta ja opiskelukykyä. Liikunnan ja kansanterveyden julkaisuja 373.
Montoye, A., Pivarnik, J. M., Mudd, L. M., Biswas, S., & Pfeiffer, K. A. (2016).Validation and Comparison of Accelerometers Worn on the Hip, Thigh, and Wrists for Measuring Physical Activity and Sedentary Behavior. AIMS public health, 3(2), 298–312.
Niemi, J., Hakonen, H., Lindfors, H., Tammelin, T., & Kallio, J. (2020). Koulumatkojen kulkutapaseuranta pilottikunnissa.
Ortega, F. B., Ruiz, J. R., Sjöström, M., & Castillo, M. J. (2008). Physical activity, sedentary behaviour, and metabolic syndrome in adolescents. Journal of Pediatrics, 152(6), 835-838.
Rosenberger, M. E., Haskell, W. L., Albinali, F., Mota, S., Nawyn, J., & Intille, S.(2013). Estimating activity and sedentary behavior from an accelerometer on the hip or wrist. Medicine and science in sports and exercise, 45(5), 964–975.
https://doi.org/10.1249/MSS.0b013e31827f0d9c
Saeidifard, F., Medina-Inojosa, J. R., Supervia, M., Olson, T. P., Somers, V. K., Erwin, P. J., & Lopez-Jimenez, F. (2018). Differences of energy expenditure while sitting versus standing: A systematic review and meta-analysis. European Journal of Preventive Cardiology, 25(5), 522–538. https://doi.org/10.1177/2047487317752186
Scott, J. J., Rowlands, A. V., Cliff, D. P., Morgan, P. J., Plotnikoff, R. C., & Lubans, D. R. (2017). Comparability and feasibility of wrist- and hip-worn accelerometers in free-living adolescents. Journal of Science and Medicine in Sport, 20(12), 1101–
1106. https://doi.org/10.1016/jjsams.2017.04.017
Shi, Y., Huang, W. Y., Yu, J. J., Sheridan, S., Sit, C. H.-P., & Wong, S. H.-S. (2019). Compliance and Practical Utility of Continuous Wearing of activPALTM in Adolescents. Pediatric Exercise Science, 31(3), 363–369. https://doi.org/10.1123/pes.2018-0170
Suorsa, K., Pulakka, A., Leskinen, T., Pentti, J., Holtermann, A., Heinonen, O. J., Sunikka, J., Vahtera, J., & Stenholm, S. (2020). Comparison of Sedentary Time Between Thigh-Worn and Wrist-Worn Accelerometers, Journal for the Measurement of Physical Behaviour, 3(3), 234-243.
Telama, R., Yang, X., Leskinen, E., Kankaanpää, A., Hirvensalo, M., Tammelin, T., Viikari, J. S. A., & Raitakari, O. T. (2014). Tracking of physical activity from early childhood through youth into adulthood. Medicine and Science in Sports and
Exercise, 46(5), 955–962. https://doi.org/10.1249/MSS.0000000000000181
Tremblay, M. S., LeBlanc, A. G., Kho, M. E., Saunders, T. J., Larouche, R., & Colley, R. C. (2011). Systematic review of sedentary behaviour and health indicators in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity, 8(1), 98.
Tremblay, M. S., Aubert, S., Barnes, J. D., Saunders, T. J., Carson, V., LatimerCheung, A. E., Chastin, S. F. M., Altenburg, T. M., & Chinapaw, M. J. M. (2017). Sedentary Behavior Research Network (SBRN) – Terminology Consensus Project process and outcome. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 75. https://doi.org/10.1186/s12966-017-0525-8
Troiano, R. P., McClain, J. J., Brychta, R. J., & Chen, K. Y. (2014). Evolution of accelerometer methods for physical activity research. British Journal of Sports Medicine, 48(13), 1019–1023. https://doi.org/10.1136/bjsports-2014-093546
Tudor-Locke, C., Craig, C. L., Beets, M. W., Belton, S., Cardon, G. M., Duncan, S., Hatano, Y., Lubans, D. R., Olds, T. S., Raustorp, A., Rowe, D. A., Spence, J. C., Tanaka, S., & Blair, S. N. (2011). How many steps/day are enough? For children and adolescents. International Journal of Behavioral Nutrition and Physical Activity, 8(1), 78. https://doi.org/10.1186/1479-5868-8-78
Tuloskortti. (2018). Lasten ja nuorten liikunta Suomessa. Liikunnan ja kansanterveyden julkaisuja 345. World Health Organisation. (2020). 2020 WHO guidelines on physical activity and sedentary behaviour.
World Health Organization. (2020). Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age. https://www.who.int/publications/i/item/9789241550536.
Yang, Y., Schumann, M., Le, S., & Cheng, S. (2018). Reliability and validity of a new accelerometer-based device for detecting physical activities and energy expenditure. PeerJ, 6, e5775. https://doi.org/10.7717/peerj.5775





